Interference by insurers is driving mental health care providers to flee networks. It makes treatment hard to find. Some states are passing laws to protect patients.
Javi Sanz/Getty Images/E+
hide caption
toggle caption
Javi Sanz/Getty Images/E+
Accessing mental health care can be a harrowing ordeal. Even if a patient finds a therapist in their network, their insurance company can overrule that therapist and decide the prescribed treatment isn’t medically necessary.
This kind of interference is driving mental health professionals to flee networks, which makes treatment hard to find and puts patients in harm’s way.
ProPublica sought to understand what legal protections patients have against insurers impeding their mental health care.
This story comes from ProPublica, a nonprofit newsroom that investigates abuses of power. Sign up to receive their biggest stories as soon as they’re published.
Most Americans — more than 164 million of them — have insurance plans through employers. These are generally regulated by federal law.
Although the law requires insurers to offer the same access to mental health care as to physical care, it doesn’t require them to rely on evidence-based guidelines or those endorsed by professional societies in determining medical necessity. Instead, when deciding what to pay for, the government allows insurers to set their own standards.

“If insurers are allowed to home bake their own medical necessity standards, you can pretty much bet that they’re going to be infected by financial conflicts of interest,” said California psychotherapist and attorney Meiram Bendat, who specializes in protecting access to mental health treatment.
Federal lawmakers who want to boost patient protections could look to their counterparts in states who are pioneering stronger laws.
Although these state laws govern only plans under state jurisdiction, such as individual or small-group policies purchased through state marketplaces, experts told ProPublica they could, when enforced, serve as a model for broader legislation.
“States are laboratories for innovation,” said Lauren Finke, senior director of policy at The Kennedy Forum, a nonprofit that has advocated for state legislation that improves access to mental health care. “States can take it forward and use it for proof of concept, and then that can absolutely be reflected at the federal level.”
ProPublica reporters delved into the laws in all 50 states to determine how some are trying to chart new paths to secure mental health care access.
Many of the new protections are only just starting to be enforced, but ProPublica found that a few states have begun punishing companies for violations and forcing them into compliance.
Who defines what mental health care is necessary?
Insurers generally face few limitations on how they define what kind of mental health care is medically necessary. They often create their own internal standards instead of relying on ones developed by nonprofit professional medical societies. These standards can then be used to challenge diagnoses or treatment plans.
“Knowing the profit motive that insurers have, it’s really shocking that federal law doesn’t define medical necessity and require the use of nonprofit guidelines to make decisions,” said Bendat, who helped California legislators draft a more robust law that passed in 2020, becoming one of the first states to do so.
California’s law requires insurers to follow generally accepted standards of care for mental health and substance use conditions, forcing them to rely on evidence-based sources that establish criteria, such as nonprofit professional organizations or peer-reviewed studies. The state also barred insurers from covering only the treatment of short-term or acute symptoms, such as crisis stabilization, instead of the underlying condition, like chronic depression.
Last October, California found health care organization Kaiser Permanente in violation of the new state law and other health care regulations, reaching a settlement with the company, which agreed to pay a $50 million fine and make $150 million in investments in behavioral health care. A Kaiser spokesperson said that the company takes full accountability for its performance and that it had adopted new guidelines in line with the law. (Read their full response.)
A spokesperson for the state’s Department of Managed Health Care said the agency is auditing insurers and determining whether their networks offer enough providers to serve customers and whether they deliver timely access to care.
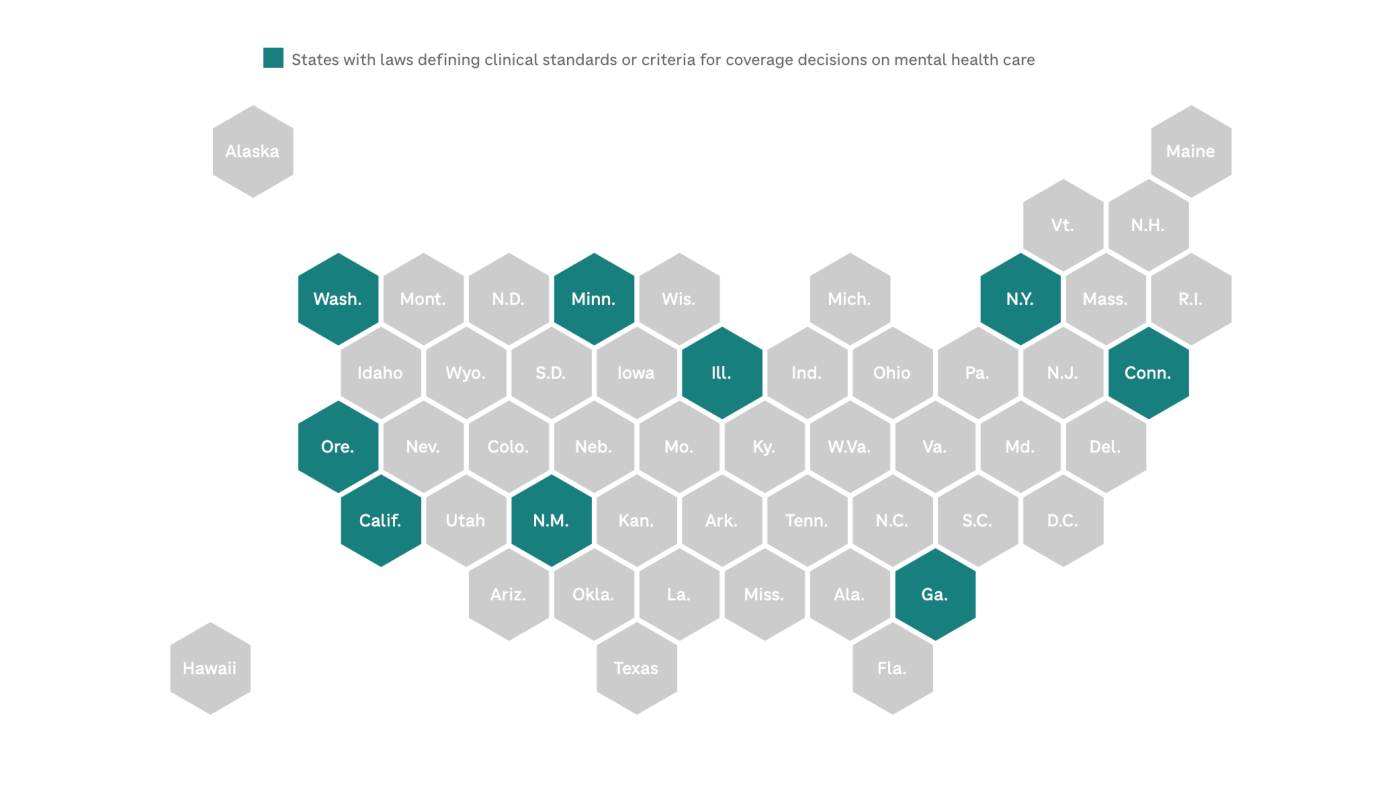
Nine states, including Oregon, Illinois and Georgia, have defined the clinical standards or criteria that insurers must use when making coverage decisions on mental health care.
Amid the opioid crisis, which has killed more than a million Americans, states have also instituted medical necessity protections for substance use treatment. For example, in Colorado, Maryland, Delaware, Connecticut and several other states, insurers must rely on guidelines from the American Society of Addiction Medicine when reviewing treatments for substance use.
How can insurers challenge mental health treatment?
Before 2008, insurance companies nationwide could put more stringent limits on how often patients got mental health care compared with medical care, instituting more restrictive caps on the number of therapy sessions per year or the length of a stay at an inpatient facility.
The federal Mental Health Parity and Addiction Equity Act banned those harder limits. So insurers shifted to a different way to deny care. “They’re not going to just cover unlimited care, so they have to do something to limit utilization,” said Tim Clement, the vice president of federal government affairs at the nonprofit group Mental Health America.
Insurers say they conduct what they call utilization reviews, in which they can request and sift through therapy progress notes full of sensitive details, to assess whether providers are delivering appropriate care. However, providers, mental health care advocates and legislators have found that these reviews are often used as pretexts by insurers looking for a reason to dispute the necessity of treatment.
In recent years, at least 24 states have passed legislation to try to regulate how insurers conduct reviews of behavioral health care.
After the New York attorney general determined that insurers, including EmblemHealth, Excellus and MVP, had violated state and federal laws with their reviews, state legislators bolstered oversight of these processes in 2019. An Excellus spokesperson said it had since adopted several reforms; MVP did not respond to ProPublica’s questions, and EmblemHealth forwarded a response from a managed health plan trade group called the New York Health Plan Association, which said that the state’s findings do not reflect the industry’s current practices. (Read their full responses.)
The New York law requires insurers to rely on criteria based on evidence and approved by the state when scrutinizing care. Peer reviewers, who work for insurance companies to assess medical necessity or appropriateness of care, must be licensed providers with relevant expertise in mental health. And when it comes to children, insurers are generally prohibited from requiring preapproval for their mental health treatment or conducting reviews during the first two weeks of an inpatient stay.
Last year, New York regulators found that Cigna’s and Wellfleet’s medical necessity criteria were out of compliance with the new law. The insurers are allowed to keep operating while they work with the state to bring their criteria in line with the law, according to the state’s mental health office. (The companies did not respond to requests for comment.)
Several states, such as Massachusetts, New Mexico and Hawaii, make insurers disclose to patients and providers the criteria or policies that they rely on for reviews.
Insurers usually select the clinician conducting reviews, but in Illinois, if there’s a disagreement about the necessity of a treatment, a patient can opt for another clinical reviewer, jointly selected by the patient, their provider and the insurer.
Some states have also limited the frequency of reviews. In Delaware, insurers are generally prohibited from reviewing inpatient substance use treatment in the first 14 days. In Kentucky and Ohio, for patients with autism, insurers cannot request more than one review annually for outpatient care.
What must insurers reveal about mental health care access?
It can be hard to enforce the laws requiring equitable coverage for mental and physical conditions; doing so entails comparing very different kinds of health care and successfully arguing there is an imbalance in access. State and federal regulators also have minimal resources for such intensive examinations, which has hindered their ability to scrutinize insurers.
To hold insurers accountable, at least 31 states and the District of Columbia have passed laws requiring them to report how much access they really provide to mental health care.
Most of these states ask insurers to provide details on their treatment criteria or limitations, but some states appear to be violating their own laws by not posting information publicly.
New Jersey’s Department of Banking and Insurance, for example, must make an insurer complaint log publicly available and post an insurance compliance report related to mental health care. But no such information has been published on its website more than five years after the state passed this requirement.
After ProPublica asked about the lack of transparency, spokesperson Dawn Thomas said that the department is working to implement the requirements and that the reporting process would begin this year. “We recognize that the reporting provisions in the law provide important public insight into compliance of carriers,” she told ProPublica in an email.
Chris Aikin, a spokesperson for the original bill’s primary sponsor, New Jersey Assembly Speaker Craig Coughlin, told ProPublica his office had been in contact with the department and would “monitor their progress to meet reporting requirements and ensure full transparency for consumers.”
For compliance reports, states often request data and analyses from insurers, but the figures that insurers submit may not be detailed or even accurate.
“I’ve reviewed a lot of these analyses,” said Clement, who has helped advocate for greater insurer transparency in multiple states, “and in most states, they’re pretty bad.”
But in some states, like Oregon, where detailed annual reporting is required, analyses revealed a disproportionate number of insurance claims for behavioral health were out-of-network compared with medical claims, suggesting that people may have faced trouble accessing therapists covered by their insurance plans.
Its reports also found that mental health providers were paid substantially less than medical providers for office visits of equivalent length. For an hourlong office visit, a mental health provider was, on average, reimbursed about half the amount given to a medical or surgical clinician. A spokesperson for the state’s Department of Consumer and Business Services told ProPublica that there have been no investigations or enforcement actions in response to the new requirements.
“There’s no way we can feel confident that anyone is following the law unless we make sure there is accountability and they have to prove that they’re accountable,” Clement said.
Other states, like New York, have begun to use the new data to drive investigations. Since 2021, the state’s Department of Financial Services has conducted nine investigations of seven insurance companies in response to the laws, according to a department spokesperson.
People can file complaints with their state insurance departments if they believe that an insurer is violating their rights.
This story comes from ProPublica, a nonprofit newsroom that investigates abuses of power.
Share your story: If you have submitted a complaint to a state insurance department that you would like to share with ProPublica reporters, reach out at mentalhealth@propublica.org.
ProPublica reviewed laws and regulations in all 50 states and the District of Columbia. If you see a state law that was not included, please send them a note.
Max Blau of ProPublica contributed research to this report. Maps by NPR’s Connie Hanzhang Jin.